
Author : USAID
Publication Type : Report
Date of publication : 2019
Link for the original document
*Wathinotes are excerpts from publications chosen by WATHI and conform to the original documents. The reports used for the development of the Wathinotes are selected by WATHI based on their relevance to the country context. All Wathinotes refer to original and integral publications that are not hosted by the WATHI website, and are intended to promote the reading of these documents, which are the result of the research work of academics and experts.
Malaria situation in Côte d’Ivoire
Côte d’Ivoire is located in West Africa, encompassing an area of 322,462 km2 . It borders Mali and Burkina Faso to the north, the Gulf of Guinea to the south, Ghana to the east, and Liberia and Guinea to the west. The political capital is Yamoussoukro, situated 248 km north of the economic capital of Abidjan. According to the 2014 General Population and Housing Census, Côte d’Ivoire’s population was 22,671,331 in 2014, and is estimated at 26,232,692 in 2018, with 51.2percent located in urban areas and 48.8percent situated in rural areas. The population density is 74 habitants/ km2 .
Forty-three percent of the total population is less than 15 years of age, and 49percent of the population is female. Women of childbearing age represent 24percent of the population, while children under 5 years of age comprise 16percent. The annual population growth rate is estimated at 2.6percent. Malaria is endemic throughout Côte d’Ivoire the whole year, with peaks during the rainy season. The rains occur in line with a sub-equatorial climate between May and July for the main season and between October and November for the secondary season, and with a tropical climate from March through May.
Côte d’Ivoire has a tropical climate with four seasons in the coastal and central regions and two seasons in the northern savannah region, including a long dry season from November to May and a wet season from June to October.
The coastal and central region has:
● a long dry season from December to May
● a short dry season from July to October
● a long rainy season from May to July and
● a short rainy season from October to November.
Country health system delivery structure and Ministry of Health (MoH) organization
The health system in Côte d’Ivoire comprises an administrative element and a care element, which are interdependent. Each has three levels, which play specific roles in malaria control. The central level, which is overseen by the Minister of Health, comprises the Cabinet, 2 General Directorates, 9 Central Directorates, 14 National Public Health Institutes and 24 Coordination Departments for the national health programs, including the NMCP. This level is responsible for defining health policy, general coordination of the healthcare system, resource mobilization, monitoring and evaluation and operational research.
In terms of care services, the central level is made up of four University Hospitals, five specialized institutions, five National Public Institutes, and the Medical Emergency Hospital. These care services provide not only treatment for severe malaria cases but also IPTp, routine distribution of ITNs, and conduct malaria-related operational research. The intermediate level represents 20 regional health departments, each of which covers several health districts, which oversee all private, public and community-level health services within their respective health region.
It comprises 18 regional hospitals, 81 general hospitals, and 2 specialized hospitals, which also provide treatment for both uncomplicated and severe malaria cases, IPTp, and routine distribution of ITNs. Amongst its responsibilities are coordination of the implementation of the national health policy and monitoring and evaluation of health activities, including malaria control interventions. The regional level hospitals serve as the first referral site for medical services that are unavailable at district level hospitals.
This FY 2018/2019 Malaria Operational Plan presents a detailed implementation plan for Côte d’Ivoire, based on the strategies of PMI and the National Malaria Control Program (NMCP) strategy.
 .
. 
National malaria control strategy The NMCP in Côte d’Ivoire was established in 1996. The previous national strategic plan covered the period of 2012-2017. This was superseded by the current plan, adopted in 2016, covering the period 2016-2020. The key aims and objectives of the National Malaria Strategic Plan 2016-2020 (NMSP 2016-2020) are presented below. The objectives of the NMSP 2016-20207 , are to: • Reduce malaria incidence by 40% by 2020 compared to 2015 baseline; and • Reduce malaria-related mortality by 40% by 2020 compared to 2015 baseline.
In the light of the aforementioned priorities, the NMSP 2016-2020 introduces a number of new key interventions: Vector Control: • Extension of routine distribution of ITNs to children from 1 year to 5 years of age
• Inclusion of prisons, orphanages, boarding schools, disability support centers, and hospitals in ITN mass distributions
• Extension of mass distribution for a period of one month following the end of the net distribution campaign in order to catch up with the population absent during the campaign Malaria in Pregnancy:
• Increase of IPTp coverage of SP from three doses to at least three doses for pregnant women during ANC clinics
• Use of SMS to improve IPTp coverage • Involvement of community health workers in provision of IPTp services to pregnant women who have missed ANC clinics 15 Case Management:
• Expansion and saturation of high impact interventions including scale-up of iCCM from 9 to 78 districts
• Provision of hospitals, mainly emergency rooms and external consultations facilities with RDTs to perform diagnostics – Systematic quality control of malaria commodities (RDTs and ACTs)
• Involvement of community health workers (CHWs) in advanced strategies to increase utilization at the community level to improving malaria diagnostics – Promote equity through advanced strategies geared to providing care to population leaving more than 5 km of health facilities
• Enrollment of private service providers in enforcing national case management directives as well as implementing no-payment policy Social and Behavior Change Communication:
• Inclusion of traditional and religious leaders in social mobilization and advocacy efforts
• Use of social networks to promote use of malaria prevention and control measures
• Involvement of local market users, unions, and truckers in disseminating messages related to malaria prevention and control.
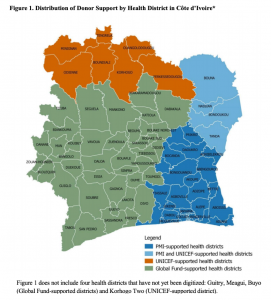
The National Malaria Control Program (NMCP) prioritizes efforts to coordinate all partners active in malaria control. Key donor and technical partners supporting the NMCP include the Global Fund, the WHO, and the United Nations Children’s Fund (UNICEF).
Under the PMI Strategy for 2015-2020, the U.S. Government’s goal is to work with PMI-supported countries and partners to further reduce malaria deaths and substantially decrease malaria morbidity, towards the long-term goal of elimination. Building upon the progress to date in PMI-supported countries, PMI will work with NMCPs and partners to accomplish the following three objectives by 2020:
- Reduce malaria mortality by one-third from 2015 levels in PMI-supported countries, achieving a greater than 80% reduction from PMI’s original 2000 baseline levels.
- Reduce malaria morbidity in PMI-supported countries by 40% from 2015 levels.
- Assist at least five PMI-supported countries to meet the World Health Organization’s (WHO) criteria for national or sub-national pre-elimination.
Commenter